
One-Size-Fits-All Caps Cause Damage
- Hairline Illusions

- 16 hours ago
- 7 min read

A wig cap is not a hat.
It is a prosthetic interface that sits in direct, continuous contact with compromised human tissue. Every element of its construction, from the base material and ventilation pattern to the weight distribution and adhesive requirements, either supports the scalp beneath it or works against it. When fitting decisions are made without clinical assessment, the consequences are not hypothetical. They are physical, measurable, and often preventable.
This article examines why scalp physiology must drive cap selection for medically vulnerable clients, how different conditions create fundamentally different fitting requirements, and what the absence of clinical training costs the people we serve.
The Industry Was Built on Artistry. That Is Both Its Strength and Its Gap.
Hair replacement has a long and skilled tradition. Wig makers, ventilation artists, and custom fabricators have spent generations perfecting the visual and tactile craft of hair prosthetics. The work is genuinely technical and the aesthetic results can be extraordinary.
But the field was built around cosmetic clients. Healthy scalps. Normal skin integrity. Standard thermoregulation. The training that emerged from that tradition reflects those assumptions.
When medically vulnerable clients began seeking cranial prosthetics in significant numbers, the industry largely responded by applying the same frameworks it already knew. The caps changed in name. The clinical competency required to fit them appropriately did not always follow.
The result is a widespread practice pattern where professionals with genuine skill and good intentions are making fitting decisions they were never trained to make, for clients whose physiology they were never taught to assess.
Three Conditions. Three Physiologies. Three Different Fitting Requirements.
The three most common medical populations seeking cranial prosthetics are clients experiencing chemotherapy-induced hair loss, radiation-related hair loss, and autoimmune-related hair loss. These populations are often grouped together under the label "medical wig clients," but they present with profoundly different scalp conditions that require distinct clinical approaches.
Chemotherapy-Related Hair Loss
Chemotherapy-induced alopecia (CIA) affects approximately 65% of patients receiving cytotoxic chemotherapy, with rates varying significantly by drug class and dosage. The hair loss itself is typically temporary, but the scalp condition during and following treatment is not simply a cosmetic concern. Chemotherapy disrupts the rapidly dividing cells of the hair follicle, and the same systemic effects that drive hair loss also alter the skin's barrier function, sensitivity thresholds, and thermoregulatory capacity.
Research published in the Journal of the American Academy of Dermatology has documented increased scalp sensitivity, reduced skin barrier integrity, and compromised wound healing in patients undergoing systemic chemotherapy. Occlusive or heavy cap materials can trap heat and moisture against a scalp that can no longer regulate either effectively, creating an environment conducive to irritation, secondary infection, and tissue breakdown.
For this population, cap selection must prioritize breathability, minimal weight, and materials that do not require adhesives or fixatives that further compromise already-sensitive tissue.
Radiation-Related Hair Loss
Radiation-induced alopecia presents an entirely different clinical picture. Unlike chemotherapy, cranial radiation causes localized, often permanent follicle damage within the treatment field. But the concern extends well beyond hair loss. Ionizing radiation damages the microvasculature of the dermis and can produce fibrosis, chronic inflammation, and a progressive deterioration in skin integrity over time.
The National Cancer Institute has documented that radiation dermatitis can persist and evolve long after treatment ends, with late-stage effects including tissue atrophy, telangiectasia, and significantly impaired wound healing. Skin that has received cranial radiation is fragile in ways that are not always visible to the untrained eye. Friction, tension, and textured cap materials can create micro-trauma that this skin cannot repair at a normal rate.
For post-radiation clients, cap construction must minimize all friction and tension at the scalp interface. Lace fronts, which require some degree of movement and adhesion at the hairline, warrant careful clinical judgment in this population. The cap must protect the tissue, not simply sit on top of it.
Autoimmune-Related Hair Loss
Autoimmune alopecia, including alopecia areata and its more extensive variants alopecia totalis and alopecia universalis, presents a third distinct clinical profile. The scalp may appear intact and even healthy on visual inspection, yet be in a state of active inflammatory dysregulation at the tissue level.
Research published by the National Alopecia Areata Foundation and in peer-reviewed dermatology literature has established that alopecia areata involves T-cell mediated immune attack on the hair follicle, with disease activity that can fluctuate unpredictably. For the prosthetics fitter, this means tolerance is not stable. A client who wore a specific cap construction comfortably for months may develop sensitivity without any apparent external change. An inflammatory flare can alter the scalp environment significantly.
This population requires ongoing scalp assessment, not a single evaluation at fitting. Materials that are biocompatible and unlikely to trigger immune response deserve priority. The fitter must understand that disease activity, not just current presentation, informs the appropriate cap.

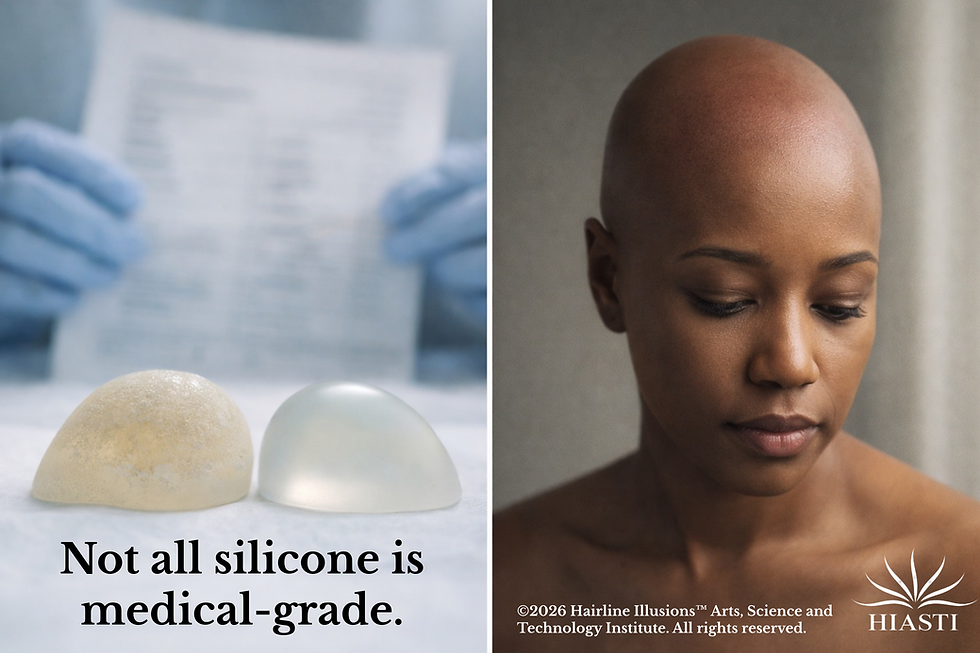
Why Silicone Grade and Lace Type Are Not Minor Details
Material selection in cranial prosthetics is not an aesthetic preference. It is a clinical determination.
Silicone, for example, exists across a broad spectrum of formulations. Industrial-grade and commercial-grade silicones contain additives, catalysts, and byproducts that are appropriate for their intended applications and not intended for prolonged contact with compromised human skin. Medical-grade silicone is governed by biocompatibility standards specifically because contact with living tissue demands a different threshold of purity and chemical stability.
ISO 10993, the international standard for biocompatibility testing of medical devices, establishes a framework for evaluating whether materials are safe for skin and tissue contact. When cranial prosthetics are manufactured using materials that have not been evaluated or selected with this framework in mind, the client bears the risk. That risk is not theoretical on a healthy scalp. It is clinically significant on a post-treatment scalp that lacks normal barrier function.
Lace carries a parallel consideration. The term "breathable" has become a marketing default in the wig industry, but breathability is not synonymous with medical compatibility. Lace has inherent texture. On intact skin with normal tactile tolerance, that texture is negligible. On skin that has been thinned by chemotherapy, fibrosed by radiation, or sensitized by autoimmune inflammation, that same texture becomes a source of chronic mechanical stress.
The stabilization methods lace requires compound the issue. Adhesives and tapes create occlusion, introduce chemical exposures, and place tension on the hairline, an area already under stress in most medical hair loss clients. Using lace without first assessing scalp integrity and tolerance is not a neutral choice. It is a risk being taken on behalf of a client who cannot evaluate it independently.
How Damage Presents, and Why It Goes Unrecognized
One of the most consequential features of cap-related scalp damage in medical clients is how slowly and quietly it develops.
Clients experiencing chemotherapy, radiation, or autoimmune hair loss are often managing significant systemic illness or chronic health challenges. Discomfort associated with a cranial prosthetic is easily attributed to the broader experience of illness. The client assumes the irritation is expected. The professional never receives feedback. The harm accumulates.
Presentations vary by population and exposure. Persistent erythema and heat in the scalp region may signal an occlusive material creating a thermal burden. Localized irritation at the hairline may indicate lace texture or adhesive intolerance. Delayed healing of minor scalp trauma may reflect radiation-related tissue compromise. Recurrent inflammatory episodes may suggest material incompatibility in an autoimmune client.
None of these presentations require a dramatic acute event to cause harm. They accumulate over time, often without connecting the cap to the symptom, and they are preventable when clinical assessment precedes fitting.
What Clinical Assessment Looks Like in Practice
Clinical cranial prosthetics fitting begins before any cap enters the conversation. Assessment is not a formality. It is the clinical act that makes every subsequent decision appropriate or inappropriate.
A proper intake for a medically vulnerable client addresses scalp integrity and current skin condition, active or recent treatment status and stage, documented sensitivities or prior reactions, thermoregulatory concerns, lifestyle and physical demands that affect the prosthetic, and the medical context of the hair loss itself.
Only after that assessment does material selection become appropriate. Only then does cap construction make clinical sense. The professional who skips this sequence and begins with "what style are you looking for" is not serving a medical client. They are serving a cosmetic client who happens to be ill.
This is the practical distinction between a service provider and a clinical practitioner, and it is a distinction that matters most to the people who have the least margin for error.
The Role of Education in Closing the Gap
The professionals most likely to cause harm to medical clients are not negligent. They are undertrained. The existing educational infrastructure for hair replacement specialists was not built with clinical competency as its foundation, and most professionals working with medical clients today received no formal instruction in scalp assessment, material science, or the physiology of medically compromised skin.
This is why continuing education in cranial prosthetics must go beyond technique and address the clinical foundations that technique serves. Professionals need to understand the biology they are working with, not just the construction methods they are applying.
HIASTI was founded specifically to address this gap. The Hair and Wig Science Series, including The Science of Cranial Prosthetics, was written to provide the foundational clinical knowledge that the industry has lacked. Because the clients who need us most deserve practitioners who were taught to the level the work actually requires.
TO CONCLUDE
There is no universal medical cap. There is only a cap that is medically appropriate for this scalp, at this moment, based on this client's clinical picture.
The assumption that one construction, one material, or one fitting approach can safely serve all medical clients is not a minor oversimplification. It is the root cause of a pattern of preventable harm that the industry rarely discusses because the field was not built to recognize it.
Raising the standard of cranial prosthetics practice begins with understanding that the cap is the least important thing in the room until the assessment is complete. Physiology comes first. Every time.
References
1. Chon SY, et al. Chemotherapy-induced alopecia. Journal of the American Academy of Dermatology.2012;67(1):e37-e47. https://doi.org/10.1016/j.jaad.2011.02.026
2. National Cancer Institute. Radiation Therapy Side Effects. U.S. Department of Health and Human Services. https://www.cancer.gov/about-cancer/treatment/types/radiation-therapy/side-effects
3. National Alopecia Areata Foundation. About Alopecia Areata. https://www.naaf.org/alopecia-areata/
4. International Organization for Standardization. ISO 10993-1: Biological evaluation of medical devices. https://www.iso.org/standard/68936.html
5. U.S. Food and Drug Administration. Use of International Standard ISO 10993-1 Biological Evaluation of Medical Devices. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/use-international-standard-iso-10993-1-biological-evaluation-medical-devices
6. Lacouture ME, et al. Skin toxicity evaluation protocol with panitumumab (STEPP), a phase II, open-label, randomized trial evaluating the impact of a pre-emptive skin treatment regimen on skin toxicities and quality of life in patients with metastatic colorectal cancer. Journal of Clinical Oncology. 2010;28(8):1351-1357.
7. Lawson, E. The Science of Cranial Prosthetics: Advanced Medical Integration and Scalp Rehabilitation. Hair & Wig Science Series, Volume 4. Hairline Illusions Arts, Science, and Technology Institute.
©2026 Egypt Lawson, All rights reserved.


Comments